
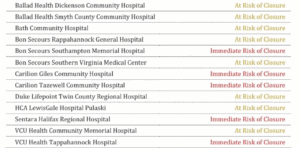
A new report by Virginia’s Joint Commission on Health Care found 13 of Virginia’s 36 rural hospitals are at distant or immediate risk of closure, as state lawmakers and their constituents work to close healthcare access gaps in the commonwealth’s farthest-flung regions.
The commission based its analysis on patients’ socioeconomic demographics and insurance types as well as hospitals’ financial information to determine risk levels for closure.
King William resident Celeste Garrett’s go-to facility, VCU Health Tappahannock Hospital, is on the list. It takes her about 20 minutes to get there and she worries about an emergency if it were to close. That would make VCU’s Richmond location her closest resource, an hour or more away “depending on the traffic.”
“Minutes matter. Seconds matter,” Franklin County resident Penny Blue said as she joined Garrett on a press call with the state’s health committee chairs Tuesday.
After a brain aneurysm in 2021, Blue was taken 15 minutes to her nearest hospital and then air-lifted to another one in Roanoke (which otherwise would have been an hour commute).
With rural hospitals already shoring up access in Southwest and South Side Virginia, the women expressed concern about themselves and their neighbors.
Some hospitals’ struggles can be traced back years and include demographics and economic regional shifts. But, the current strains are attributed to recent Medicare and Medicaid reimbursement rate cuts, a reconciliation bill Congress passed last summer that makes thousands of Virginians vulnerable to losing health insurance, and Congress’ failure to renew expired Affordable Care Act credits.
33,000 Virginians have already lost that form of insurance.
“(Rural hospitals) have always been living on the edge, but with H.R. 1 kicking in our hospitals across Virginia will lose about $2 billion dollars a year,” said Sen. Barbara Favola, D-Arlington, who chairs the Senate’s Education and Health Committee.
Uninsured people are more likely to delay care until dire situations, so hospital ERs are bracing for surges of patients. Free clinics, long considered public health safety nets, are also preparing for people to rely on them more.
“We have yet to feel the pain (of the bill) but it’s coming,” King William resident Garrett said on Tuesday’s call.
After absorbing unpaid or under-paid care from uninsured patients, health systems will eventually negotiate insurance rates with private insurers. This may lead to higher premiums for people with private insurance down the line, health systems have warned.
Sentara chief administrative operator Aubrey Layne said in a recent phone call that the hospital chain has become “more purposeful lately about getting the public to understand” the challenges.
That chain has facilities around the state, with its Sentara Halifax Regional Hospital on the new at-risk list.
Still, Virginia Hospital and Healthcare Association spokesman Julian Walker said hospitals will continue to adapt rather than close overnight or forever.
“We will see what other measures might have to be taken to continue to sustain hospitals longterm,” he said.
Those efforts are already playing out in some cases. Citing Congress’ bill as a contributing factor, Valley Health changed staffing contracts and trimmed services this spring. Last winter, Centra closed its labor and delivery unit at a hospital in Farmville. Last fall, Shenandoah Valley’s Augusta Health closed three clinics.
House Health and Human Services chair Del. Rodney Willett, D-Henrico, emphasized that the federal government placed heavy burdens on state and local governments, calling it a “situation no one wants to be in.”
The state’s pending budget has proposals to help the state comply with additional requirements for Medicaid and Supplemental Nutrition Assistance Program verifications and could support a state-level ACA subsidy to plug some holes.
Favola and Willett said the efforts cannot fully heal what federal actions have created but are a reflection of bipartisan assistance.
As both lawmakers have served on bipartisan health-focused committees and commissions, Willett said Congressional Republicans should be held accountable for pushing through the reconciliation bill but that going forward, both parties will have to work together to create lasting solutions.
“This report is a nonpartisan report done by the joint commission, we all sit on that — Republicans and Democrats,” Willett said. “The facts are the facts and what’s being done to us by Washington is unconscionable.”
